Stakeholders Meeting-Geriatric Transitional Care

Hello, and thank you for attending this stakeholders meeting. Today, we will discuss an issue that was problematic to the healthcare facility and how the inter-collaboration of professionals resolved the same. In this presentation, I will discuss the organizational/patient matters that affected the healthcare facility and, more specifically, the ED and the in-patient ward, the planned change model that was used, and how the success of the plan was evaluated.
I want to start by acknowledging the good work you have all done. As you recall, a few months back, we were in a crisis of sorts. It is because of our input that we are now able to serve the senior patient population with efficacy and effectiveness.
In our midst today, we have :
- ED and ward nurses
- Physicians
- Specialists, including oncologists and diabetes experts
- Nutritionist
- IT representative
- Clinical Nurse Leader
The main issue that the healthcare facility faced was transitioning care of elderly patients. The specific problematic areas were the admission transition of geriatric patients for acute care from a nursing home to the healthcare facility or from a home-based care service. The second and linked area was the discharge transition from the healthcare facility to the home-based services or nursing home from the healthcare facility.
The approach that the leadership took was reactionary rather than preventive. For example, a geriatric patient with hypertension and diabetes would be brought from home-based care with anemia, fatigue, loss of appetite, and weakness. The carer would assure the admitting nurses that the patient had been consistent with their medication adherence. However, on performing lab exams on the patient, it was discovered that the patient had developed renal failure due to high blood glucose levels. The hospital would then take a reactionary approach and treat the patient and later discharge the patient to the same carer. This strategy was not working, and something needed to be done.
Elderly patients often have multiple care needs due to polypharmacy, cognitive impairments, physical disabilities, and chronic diseases. Moving such patients through various levels within the healthcare facility and across healthcare settings increased the risk of the patients receiving fragmented care, and some would experience adverse events because of such things as confusion concerning their medication, failure for care follow-up, and inadequate preparation for the patient and the carer for transitional care.
Effective transitional care can help in mitigating medical errors as well as identify issues that can be addressed through early intervention. Additionally, the transition of care can also avert unnecessary readmissions and hospitalization, offer support to the choices and preferences of patients, and avoid service duplications. Consequently, effective change of care can improve the quality of care while simultaneously utilizing resources.
An ideal care transition is founded on a comprehensive plan of care and the availability of practitioners who are well-trained in their area of specialty and who also have current information on the clinical status, health status, preferences, and treatment goals of their patients. The healthcare facility, in this case, was delivering fragmented care to elderly patients, which resulted in poor patient outcomes. When a patient was admitted, the specialist at hand would cater to the patient’s medical needs until such a patient moved to the next specialist, was accepted, or was discharged. The specialists did not communicate with each other on the progress of the patients but rather relied on the EHR notes.
Transitional care coordination was necessitated for better results, increased care efficiency, and elimination of adverse events and medical errors.
Working as a team helped first to eliminate fragmented communication. The team members, for the first time, were able to be in one meeting and discuss the issues they had faced with caring for geriatric patients.
Each specialist pointed out the specific issues they faced. For example, the cardiac specialist mentioned that often, he did not know whether his patients were adhering to the requirements of the nutritionist. The diabetes specialist pointed out that he did not also know whether the nurses had given sufficient education to the patient regarding glucose monitoring and if the patient was adhering to the instructions provided to them.
As a team, the interdisciplinary approach helped in face-to-face and open communication rather than simply relying on the EHR. A single patient was cared for by one complete team that followed the patient from admission to discharge and afterward. In this way, the patient received holistic and comprehensive care from a coordinated team
The main objectives of the interdisciplinary plan were to:
- Improve geriatric patient care
- Remove silos in patient care
- Reduce hospital readmissions
- Reduce hospitalizations
- Reduce duplication of care for geriatric patients
The plan was likely to work because, first, all participants realized the need to improve the care given to geriatric patients. The nurses were rather apprehensive about the new plan as they felt that it would increase their workload. However, persuasion from the CNL and the pointing of a change agent soon changed the nurses’ attitude. It was agreed that communication between the team members needed to be frequent and open. Hence, the CNL held two meetings in a week to update each member on the progress of the plan.
The Clinical Nurse Leader took the lead in the proposed change and implemented the Planned change theory.
The seven steps in the planned theory of change include problem diagnosis; change system capacity and motivation assessment; change agent motivation and resources assessment; change strategies and objectives’ establishment; determining the change agent’s role; maintaining the change; and the gradual termination of help as the difference becomes fully absorbed in the organization’s culture (Laveneziana, 2020).
Interdisciplinary collaboration at the healthcare facility was a new concept prior to the recent changes that were made in transitional care. Initially, staff wanted to work in their areas of expertise, which made care to be fragmented. The concept of interdisciplinary collaboration had not been introduced, and when it finally was introduced, some resisted the idea. Some staff believed that having such a team would require for them to spend more time than they normally would on a patient.
The first step was to make aware the nursing staff of the existing problem that the healthcare facility had with the elderly patients’ admission and discharge. Nurses in the ED were called for a meeting, and this issue was raised. The CNL pointed out that the hospital staff needed to follow up on this category of patients to reduce the readmission and hospitalization rates. Nurse buy-in was necessary, and hence, the CNL assured the nurses that their workload would not increase but rather, in the long term, their workload would, in fact, decrease once the system was in place.
The CNL elected a change agent among the nurses who would be affected by the new change. The change agent acted as the motivator and was trained to respond quickly to the concerns of the nurses once the difference was in place (Rafferty, 2018). So, while the CNL would oversee the entire project, the change agent was at the most basic level of ensuring change was assimilated by all affected staff. The CNL also created objectives for the change and simplified them such that each nurse would easily remember them and work towards achieving the same. The goals were made step-wise-wise manner so that the staff would not feel overwhelmed when trying to meet the objectives.
The physicians, the specialist, the nurses, and the geriatric patients and their carers needed to collaborate for better patient outcomes. The gap in care was mainly because ofollow-up follow-up, fragmented care, and lack of communication. When geriatric patients reported to the healthcare facility, they were required to have the history of their illnesses with them; this was often not possible. However, with the new change model, the CNL tasked nurses at the ED to create health passports for every geriatric patient who was admitted to the hospital (Jubraj et al., 2016). The health passport included the history of past and current illnesses, a list of all specialists that the patient had visited, current medications, current specialists, and current care they were receiving. The digital health passport also contained information about the carer’s name and address. The change required that once a patient was admitted and all details uploaded in the health passport, the specialists at the healthcare facility would be informed of the patient’s information, and these would schedule the patient as per the requirements of the illness. After discharge, the nurses at the ED were tasked with following up on the patient, giving the carer and the patient education on how to care for the patient, and a contact number that either of the two would call; the same number would be used to call the two to check up on the patient and to ensure that they were adhering to the treatment protocols they had learned.
The change did not require a significant financial budget. The difference mostly needed time to be allocated to following up on the patients. The department had four additional telephone line extensions added to the department floor that were dedicated to calling and following up on the patients. The IT department created the digital health passports.

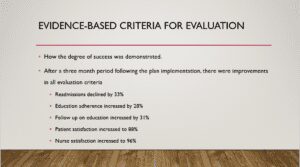
Successful outcomes would be reduced patient hospitalizations, reduced readmissions, and increased patient satisfaction.
The success of the project needed to be evaluated. To do so, the CNL required that the number of geriatric patients who visited the hospital on admission be correctly documented and their health passports created and updated.
The CNL also analyzed the data to determine how many readmissions had occurred after the plan was implemented. Another parameter that was used was the patient’s adherence to their medication and nurse education. The nurses who were tasked with following up on patients were required to enter information on the progress as regards patient medication adherence and how well a patient was keeping in line with the instructions they had received upon discharge. The next parameter was nurse and patient satisfaction. The patients were asked to fill in a questionnaire after three months to determine their level of satisfaction with the new plan. Nurses, too, filled out a survey questionnaire. In the questionnaire, the nurses gave their feedback on the project, including what they liked and did not like, suggestions for improvement, and their level of satisfaction with the program.
In conclusion, the planned change was successful. The healthcare facility was aware that transitional care for its geriatric patients needed to improve if better patient outcomes were to be achieved. We needed to take a preventive rather than a reactionary approach. The interdisciplinary team that was created was efficient in its service delivery. Any hiccups were quickly resolved. I would like to especially appreciate the nurses who, through the change agent, were able to embrace the project to make it a success. Lastly, the data discussed herein summarizes the improvement markers in service delivery as well as nurse and patient satisfaction. We shall have another evaluation after three months. We believe that the patient outcomes will supersede what we have currently achieved.
ORDER A PLAGIARISM-FREE PAPER HERE
We’ll write everything from scratch
Question 
For this assessment, you will create an 8-12 slide PowerPoint presentation for one or more stakeholder or leadership groups to generate interest and buy-in for the plan proposal you developed for the third assessment.
Stakeholders Meeting-Geriatric Transitional Care
As a current or future nurse leader, you may be called upon to present to stakeholders and leadership about projects that you have been involved in or wish to implement. The ability to communicate a plan—and the potential implications of not pursuing such a plan—to stakeholders effectively can be critically important in creating awareness and buy-in, as well as building your personal and professional brand in your organization. It is equally important that you know how to create compelling presentations for others and ensure that they convey the same content you would deliver if you were the presenter.
You are encouraged to complete the Evidence-Based Practice: Basics and Guidelines activity before you develop the presentation. This activity consists of six questions that will create the opportunity to check your understanding of the fundamentals of evidence-based practice as well as ways to identify EBP in practice. The information gained from completing this formative will help promote success in the Stakeholder Presentation and demonstrate course room engagement—it requires just a few minutes of your time and is not graded.
Demonstration of Proficiency
Competency 1: Explain strategies for managing human and financial resources to promote organizational health.
Explain how the interdisciplinary plan could be implemented and how the human and financial resources would be managed.”<li”>Competency 2: Explain how interdisciplinary collaboration can be used to achieve desired patient and systems outcomes.
Explain an organizational or patient issue for which a collaborative interdisciplinary team approach would help achieve a specific improvement goal.
Competency 3: Describe ways to incorporate evidence-based practice within an interdisciplinary team.
Summarize an evidence-based interdisciplinary plan to address an organizational or patient issue.
Propose evidence-based criteria that could be used to evaluate the degree to which the project was successful in achieving the improvement goal.
Competency 5: Apply professional, scholarly, evidence-based communication strategies to impact patient, interdisciplinary team, and systems outcomes.
Slides are easy to read and error-free. Detailed speaker notes are provided.
Organize content with clear purpose/goals and with relevant and evidence-based sources (published within five years) with an APA formatted reference list with few errors.
Professional Context
This assessment will provide you with an opportunity to sharpen your ability to create a professional presentation to stakeholders. In this presentation, you will explain the Plan-Do-Study-Act cycle and how it can be used to introduce the plan (P), implement the plan (D), study the effectiveness of the program (S), and act on what is learned (A) to drive continuous improvement nt. By using this cycle, the stakeholders will have a tool and a proposal to expand on these ideas to drive workplace change and create improved processes to solve an interprofessional collaboration problem.
Scenario
In addition to summarizing the key points of Assessments 2 and 3, you will provide stakeholders and leadership with an overview of project specifics as well as how success would be evaluated. You will essentially be presenting a discussion of the Plan, Do, and Study parts of the PDSA cy le. Again, you will not be expected to execute the project, so you will not have any results to study. However, by carefully examining the ways in which your plan could be carried out and evaluated, you will get some of the experience of the thinking required for PDSA.
When creating your PowerPoint for this assessment, it is important to keep in mind the target audience: yinterviewee’see’s organizational leaders ip. The overall goal of this assessment is to create a presentation that your interviewee could potentially give in their organization.
Instructions
Please follow the Capella Guidelines for Effective PowerPoint Presentations [PP X]. If you need technical information on using PowerPoint, refer to Capella University Library: PowerPoint Presentations.
Be sure that your plan addresses the following, which corresponds to the grading criteria in the scoring guide. Please study the scoring guide carefully so you understand what is needed for a distinguished score.
Explain an organizational or patient issue for which a collaborative interdisciplinary team approach would help achieve a specific improvement goal.
Summarize an evidence-based interdisciplinary plan to address an organizational or patient issue.
Explain how the interdisciplinary plan could be implemented and how the human and financial resources would be managed.
Propose evidence-based criteria that could be used to evaluate the degree to which the project was successful in achieving the improvement goal.
Communicate the PowerPoint presentation of the interdisciplinary improvement plan to stakeholders in a professional manner, with writing that is clear, logically organized, and respectful, with correct grammar and spelling using current APA style.
There are various ways to structure your presentation; the following is one example:
Part 1: Organizational or Patient Issue.
What is the issue that you are trying to solve or improve?
Why should the audience care about solving it?
Part 2: Relevance of an Interdisciplinary Team Approach.
Why is using an interdisciplinary team relevant, or the best approach, to addressing the issue?
How will it help to achieve improved outcomes or reach a goal?
Part 3: Interdisciplinary Plan Summary.
What is the objective?
How likely is it to work?
What will the interdisciplinary team do?
Part 4: Implementation and Resource Management.
How could the plan be implemented to ensure effective use of resources?
How could the project be managed to ensure that resources were not wasted?
How does the project justify the resource expenditure?
Part 5: Evaluation.
What would a successful outcome of the project look like?
What are the criteria that could be used to measure that success?
How could this be used to show the degree of success?
Again, keep in mind that your audience for this presentation is a specific group (or groups) at yinterviewee’see’s organization, and tailor your language and messaging accordingly. Remember, also, that another person will ultimately be giving the presentation. Include the thorospeaker’s notes that flesh out the bullet points on each slide.