Solution-Focused Therapy vs. Reality Therapy
In addiction treatment, therapists utilize various approaches to guide clients toward recovery. Among these, solution-focused therapy and reality therapy offer distinct methodologies for achieving positive change. Although both are pursuits of helping people to deal with issues of the self, some distinct features set one from the other as far as methodology and the role of the practitioner are concerned: Solution-Focused Therapy vs. Reality Therapy.
This paper aims to compare solution-focused therapy and reality therapy, describing the theoretical background of both approaches, the stages of treatment, ways to encourage a client’s recovery, and how to address any challenges that may arise in the process of counseling. Moreover, it will analyze the position of the human service provider in each therapy and further compare and contrast them in detail.
Theories Overview
Solution-Focused Therapy
Solution-focused therapy (SFT), developed by Steve de Shazer and Insoo Kim Berg, is a therapeutic approach that emphasizes goal-oriented and future-focused interventions. The central premise of SFT is based on the belief that clients have the capabilities and assets needed to solve their problems. The role of the therapist is to assist clients in identifying useful strategies derived from these inner resources in looking for workable solutions to the problem (Cooper et al., 2024).
Hence, SFT concentrates more on making goal-oriented, specific, and realistic behavior changes that a client can start adopting in the present. The theory does not involve looking at a different phase or ailed conditions of any individual and does not diagnose but reframe or enhance the resource to enable the client to take up the responsibility of reconstructing their life.
Reality Therapy
Reality therapy, founded by William Glasser, is based on Choice Theory, which asserts that human behavior is driven by the need to fulfill five basic needs: survival, love and belonging, power, freedom, and fun. This theory posits that one is capable of deciding how to meet those needs and that taking personal responsibility is the determinant of change (Nunez, 2020).
In reality therapy, the therapist makes joint efforts with the client to recognize some behaviors that seem not to be satisfactorily meeting these needs and assist the client in finding ways to make appropriate behaviors and choices that can produce more useful and satisfying outcomes. It does not involve uncovering past incidences or issues and instead centers its attention on current decisions and actions.
Comparison of Theoretical Concepts, Principles, and Agents of Change
Similarities
Both solution-focused therapy and reality therapy emphasize client empowerment, encouraging individuals to take control of their lives. They are both prospective in that they are both proactive and geared to cause change for the better besides recounting other incidents that may have happened in the past.
Every approach pays attention to the client’s ability to change and sees the therapist as an accompanying assistant. Second, both theories focus on the client’s responsibility for the recovery, stressing the point that clients play a significant role in their recovery process. Small build-up changes are more effective for sustainable development and transformation, along with self-efficacy and organizational resilience.
Differences
The key difference between the two therapies lies in their foundational concepts. SFT focuses on identifying solutions based on the client’s existing resources and strengths, whereas reality therapy theory is based on the Choice Theory, which involves the human needs that are fundamental to people.
In reality therapy, however, clients are helped to improve on the decisions that they make to meet their needs and to make better choices, while solution-focused therapy focuses on the building of solutions without exploring the need that may have led to the behavior. In SFT, the therapist’s task is mainly to help the client find the solution oneself, while in reality theory, the therapist directs the client on how to assume responsibility for their decisions and behavior.
Stages Associated with Treatment
Similarities in Treatment Stages
Both therapies follow a structured process that includes a beginning phase, where the therapist establishes a rapport with the client and identifies the problem or issue at hand. The treatment then moves to the middle phase, where the therapist and the client identify solutions and pathways toward solving the problem. The third phase is the collaborative phase, in which the therapist works with the client to come up with new ways of using their strengths to address problems (Opland & Torrico, 2024).
In sum, both therapies have a termination stage, in which the therapist and the client identify and discuss what has been achieved, as well as discuss how the change that has been made in the course of the therapy will be sustained. This is a critical step to maintain the progress of the client toward long-term recovery.
Differences in Treatment Stages
In solution therapy, the stages are more clearly defined, beginning with goal-setting, followed by identifying exceptions to the problem, and then ending with solution-building. The cognitive solution relies on simple steps that can be made in the client’s daily life and reality. On the other hand, there is no sequential set of reality therapy that needs to be followed by one. The assessment of the client’s needs is active and occurs during the first session only, whereas the therapeutic process itself is more active, and the therapist helps the client evaluate and modify their decisions and actions.
In reality therapy, the therapist does not follow any protocol of stages but interacts with the client and plans out their actions and reactions, which may change on an ongoing basis. Priority needs refer to those that are more critical than the other basic needs and which, if not met, can cause more injuries or harm to the client compared to other needs.
Creating Positive Change to Promote Recovery
Similarities
The two therapies focus on creating positive change by helping the client identify what is already working in their life and building on it. In solution-focused therapy, the client is guided by the therapist to explore and magnify specific aspects of the problem that are lacking or were much less severe or nonexistent (Jerome et al., 2023). In reality therapy, the role of a therapist is to assist a client in finding out issues that they have chosen and the behaviors that are not useful to them and help them to make better choices and to get other, more useful options.
Differences
In SFT, positive change is primarily achieved by identifying small, manageable steps that can lead to larger transformations. Emphasis is on what should be done instead of what is wrong or what went wrong. In reality therapy, the focus is on choices and responsibility.
The therapist helps the client define how the current behaviors and choices interfere with the ways of fulfilling their needs and assists the client in finding ways of making more effective choices. Nevertheless, the two therapies focus on empowering the client; however, reality therapy is more dependent on the client first making some key behavioral changes.
Approaching Obstacles in the Treatment Process
Similarities
Both therapies postulate that obstacles are a natural part of the treatment process and must be addressed by helping clients recognize what is working and what is not. Both therapies are client-centered and promote a positive attitude and recollection of previous strengths in coping ability. They help clients develop confidence and self-reliance in tackling future challenging situations. In SFT, the therapist will assist the client in identifying the wished-for outcome and looking for times when the problem was not all that large.
In reality therapy, the therapist has to look at how the client may be preventing them or encourage them to make better choices if things are preventing them from getting where they want to be. While both therapies involve the client taking responsibility for the issues and working toward managing these, these therapies also involve the client’s skills and abilities in equal measure.
Differences
In SFT, obstacles are often addressed by highlighting exceptions—times when the problem was less intense or absent—and using these exceptions as the basis for creating solutions. This enables clients to understand their achievements and adapt them to future behavior. In reality therapy, problems are construed as consequences of wrong decisions and the therapist assists the client to look at the choices that have been made and the outcomes that follow. While in therapy, Carl Rogers leans more toward the inner barriers within the client and encourages the person to look inside (Yao & Kabir, 2023).
However, SFT focuses on the outside presentation and problem-solving approach to direct the client toward practical solutions that exist in the current and future. Nevertheless, both approaches motivate the client to make balanced changes; however, SFT focuses on the external circumstances, while reality therapy targets the internal reasons behind the difficulties.
The Human Service Provider’s Role
Similarities
In both therapies, the therapist plays a collaborative role in the client’s recovery process. Both approaches consider the therapist as an observer who assists the client in discovering the strengths that can enable change. The role played by the therapist involves helping the client make proactive approaches to solve the problem and start the recovery process.
It also builds rapport and trust from the side of the therapist while ensuring that the client is in control of their choices and actions (Wampold & Flückiger, 2023). This partnership promotes confidence in the process and enables the client to take responsibility for the progress. In this way, both therapies establish the notion of therapeutic rapport that enables clients to address their concerns and achieve sustainable change.
Differences
The therapist’s role in SFT is that of a facilitator who helps the client find their solutions. This process helps the client use the insight effectively and independently without a prescription from the therapist. However, in reality therapy, the role of a therapist is more active as they guide the client through the process.
The role of a therapist is to help the client identify their needs and then assist them in coming up with a better way of fulfilling the identified needs. Although both are client-oriented, reality therapy uses a more directive and coaching style, whereas SFT focuses on the client’s ability to create solutions.
Additional Noteworthy Similarities and Differences
Integration Potential
Solution-focused therapy and reality therapy are both versatile and can be employed in different client situations. They both focus on the capability of the client to make practical changes in their lifestyles. The incorporation of solution-focused brief therapy along with reality therapy may offer a useful framework for treating clients with addictive disorders to provide rich solution-based and need-based perspectives on the client’s responsibility. For instance, clients may begin with SFT to set reactive and realistic plans, then progress to reality therapy to embrace personal accountability in attaining the set targets (Nunez, 2020).
Flexibility and Adaptability
Both therapies can be implemented individually or in combination and are appropriate for various therapeutic environments. SFT is applied in brief therapy contexts because it is goal-oriented with a focus that is appropriate for brief therapy approaches. It is particularly used when clients require rapid alteration or where transference is a planned short-term treatment. Reality therapy, however, is more time extensive and is used with clients who need to reflect on their decisions and actions. Notably, both therapies can be used for either individual or group interest, while reality therapy might take more time to implement.
Conclusion
Solution-focused therapy and reality therapy offer valuable perspectives on facilitating behavior change. While SFT enhances solution-building approaches that are strength-based, reality therapy focuses on responsibility and intrapersonal requirements that dictate behavior. Nonetheless, both therapies enable clients to regain control of their lives and make informed decisions for the betterment of themselves and their recovery. A clinician can understand the differences between each approach and determine one that will be best suited for the client, the context of the therapy, and the client’s needs and goals.
References
Cooper, Z. W., Mowbray, O., Ali, M. K., & Leslie. (2024). Addressing depression and comorbid health conditions through solution-focused brief therapy in an integrated care setting: a randomized clinical trial. BMC Primary Care, 25(1). https://doi.org/10.1186/s12875-024-02561-8
Jerome, L., McNamee, P., Abdel-Halim, N., Elliot, K., & Woods, J. (2023). Solution-focused approaches in adult mental health research: A conceptual literature review and narrative synthesis. Frontiers in Psychiatry, 14(1068006). https://doi.org/10.3389/fpsyt.2023.1068006
Nunez, K. (2020). Reality therapy techniques, benefits, and limitations. Healthline. https://www.healthline.com/health/reality-therapy
Opland, C., & Torrico, T. J. (2024, October 6). Psychotherapy and therapeutic relationship. Nih.gov; StatPearls Publishing. https://www.ncbi.nlm.nih.gov/sites/books/NBK608012/
Wampold, B. E., & Flückiger, C. (2023). The alliance in mental health care: conceptualization, evidence, and clinical applications. World Psychiatry, 22(1), 25–41. https://doi.org/10.1002/wps.21035
Yao, L., & Kabir, R. (2023, February 9). Person-centered therapy (Rogerian therapy). PubMed; StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK589708/
ORDER A PLAGIARISM-FREE PAPER HERE
We’ll write everything from scratch
Question 
Written Assignments 2
Students will be required to complete two papers during the 8 week module. Your first paper is due at the end of Unit 4 (59373) and the second paper is due at the end of Unit 7.
Rubrics will be used to grade your work. Assignments should be written in the format of the most current edition of the APA manual. Each paper must be submitted via Blackboard (Safeassign link in unit) and emailed copies will not be accepted. Please use a Microsoft Word format to submit papers (no PDFs or other programs please). Policies in regard to turning work in late also apply to these assignments.
Each written assignment will consist of a paper that is at least 6 full pages. Each paper must be double spaced with size 12 Times New Roman font and 1 inch margins on all sides. You will need to follow the example provided under course information and need a title page, body (at least 6 full pages), and reference section all in APA style.
Please use complete sentences, appropriate grammar, spelling, and references. You will also be required to use in-text references in your work in accordance with APA style to avoid plagiarism. Information to help with your writing is provided under the APA resources section of the course information tab.
Please be sure to avoid using internet sources such as Wikipedia or other web-based resources that do not have strong academic backing. You must use at least 3 additional scholarly sources not used in this course. Plagiarism detection software will be used to scan each paper and any paper that is determined to have academic integrity issues will earn a score of 0 automatically.
Students are encouraged to use University support services for writing and review closely all information in regard to academic integrity.
DO NOT REUSE ANY INFORMATION FROM THIS OR ANY COURSE IN YOUR PAPER (e.g. discussion board contributions OR information about a theory used in a previous paper)
Solution-Focused Therapy vs. Reality Therapy
Paper Topics:
NOTE: You cannot resubmit any previously written information on your WA #1 when turning in WA #2. This is not allowable and considered an academic integrity and University violation.
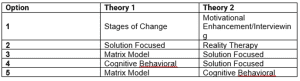
For each paper, please choose an option # (listed above on the graph) for your first paper and another for your second.
After choosing an option, please provide a brief (1 paragraph for each theory) summary of the key aspects of the theory. Afterwards, please COMPARE and CONTRAST the
two theories chosen by addressing the following:
- • Similarities and differences in general theoretical concepts, principles, and agents of change
- • Similarities and differences in stages associated with treatment according to teach theory (e.g. beginning, middle, and termination stages, etc.)
- • Similarities and differences in creating positive change to promote recovery through the concepts of the theories.
- • Similarities and differences in approaching obstacles in the treatment process.
- • Similarities and differences in the human service provider’s role in the treatment process.
- • Other similarities and differences in the treatment process that are noteworthy
Please title your paper listing the names of both theories such as, “Matrix Model vs. Solution Focused Therapy.
Readings:
- Please read Stevens & Smith (2018)
- Please read information about each of the 12 steps (1-12) listed by clicking HERE. Additionally, you could benfit from listening to any of the audio sections which are included through this website if you choose but it is not required.
- Please read information about the Minnesota Model by clicking HERE (read pages 111-113).
- Please read that article discussing the myths and misconceptions of self help groups by clicking HERE