Pilot Plan Template – Root-Cause Analysis
Create a pilot plan in response to the VOC report found in the course using this template.
Perform a root-cause analysis by doing the following:
- Critique the continuous quality improvement (CQI) team’s five whys analysis by explaining how it could have been conducted more effectively.
The Five Whys analysis is a straightforward yet powerful tool for identifying the root causes of a problem by repeatedly asking the question “Why?” until the fundamental cause is uncovered. However, the CQI team’s application of this analysis could have been more effective in the following ways:
|
Discuss whether the “why” cycle has been performed to a logical end in which additional questions would not change the response.
| In a well-conducted Five Whys analysis, the cycle should reach a point where asking additional “Why?” questions no longer adds value or uncovers new information. However, in this case, the cycle may have stopped prematurely. The root causes of doctor-patient communication issues could involve factors like time constraints, insufficient training, or even a cultural gap, which may require asking deeper questions about hospital practices and individual staff behaviors. As for pain management, addressing the issue of patient dissatisfaction involves understanding not just the administration of pain relief but also the patient triage process, nurse responsiveness, and protocol adherence.
Therefore, the CQI team should have continued to dig deeper into both systemic and cultural issues until all root causes were fully identified. Additionally, it’s critical that the team continuously cross-checks findings with data (e.g., VOC survey data) and real-time observations to ensure the Five Whys method reaches a logical conclusion. |
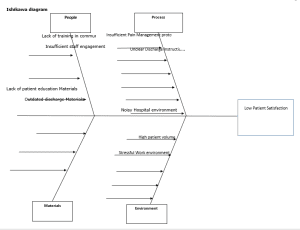
- Using the template below, create an Ishikawa diagram using the information from the SIPOC Process diagram from Task 1 and the five whys analysis.
- Explain the effectiveness of using the Ishikawa diagram to synthesize the results from multiple information sources.
|
The Ishikawa diagram provides an effective tool to visualize how multiple factors contribute to low patient satisfaction. It allows for a comprehensive view of the problem, highlighting the interdependencies between people, processes, materials, and environmental factors. Synthesizing information from both the SIPOC diagram and the Five Whys analysis helps pinpoint areas requiring immediate intervention and informs the development of improvement strategies. |
- Discuss the assumptions that you made about the organization, its processes, or both to complete the Ishikawa diagram.
|
- Using the information from the root-cause analysis in part A (e.g., the five whys analysis and the Ishikawa diagram) and the previously completed project charter from Task 1, do the following:
- Identify three opportunities for improvement.
|
1. |
Doctor-Patient Communication |
|
2. |
Pain Management |
|
3. |
Clarity of Post-Discharge Information |
Recommend one improvement strategy for each of the three opportunities identified in part B1.
| Opportunity | Improvement Strategy |
| Doctor-Patient Communication | Implement a comprehensive communication training program for all physicians and nursing staff that includes techniques for empathetic listening, cultural competency, and treatment transparency (Ha & Longnecker, 2010). The program should include role-playing and feedback mechanisms to ensure effective implementation. |
| Pain Management | Standardize pain assessment protocols across all departments, using tools like the Visual Analog Scale (VAS) or Numeric Rating Scale (NRS) to ensure that pain management is proactively addressed. This includes training for nurses and physicians on timely pain relief administration, particularly in triage situations (Ahmadi et al., 2016). |
|
Clarity of Post-Discharge Information |
Develop personalized discharge instructions for every patient, considering their individual medical conditions and needs. This should be complemented by a post-discharge follow-up system, where patients receive a call or text to clarify any doubts about their care (Jack et al., 2009). |
- Create an improved process flowchart that represents what an ideal process might look like considering the current Shelbyville Medical Center model from Task 1.
+——————————-+
| Patient Admission |
| (Triage) |
+——————————-+
|
v
+———————————————+
| Initial Assessment |
| (Identify Caregiver, Set Goals, etc.) |
+———————————————+
|
v
+———————————————+
| Daily Rounds & Education |
| (Teach-back, Medication Review, etc.) |
+———————————————+
|
v
+———————————————+
| Discharge Planning |
| (Schedule Meetings, Provide Checklists, |
| Confirm Next Steps) |
+———————————————+
|
v
+———————————————+
| Discharge Meeting |
| (Review Instructions, Confirm |
| Understanding) |
+———————————————+
|
v
+———————————————+
| Final Discharge |
| (Provide Materials, Arrange Follow-Up) |
+———————————————+
|
v
+———————————————+
| Post-Discharge Follow-Up |
| (Phone Call to Confirm Understanding)|
+———————————————+
- Create a pilot implementation plan based on information obtained in parts A and B:
| Pilot Plan | |
| Three process changes that will potentially affect the causal factors driving low patient satisfaction | 1. Doctor communication training
2. Standardized pain management protocol 3. Personalized post-discharge instructions and follow-up
|
| Affected departments or services | Medical and Nursing Staff
Emergency Care, Pain Management, Nursing Nursing, Patient Education, Discharge Coordination |
| Timeline of the projected pilot implementation plan for the process changes | 3-6 months with monthly progress reviews and evaluations. Implementation begins in 1 month. |
| Key metrics relevant to the three process changes that will be measured | 1. Doctor-Patient Communication Satisfaction Score (Goal: ≥82%)
2. Pain Management Satisfaction Score (Goal: ≥85%) 3. Patient Understanding of Discharge Instructions (Goal: ≥60%) |
| Explain how improvement from the baseline will be defined | Improvement will be defined as a percentage increase in patient satisfaction and understanding in all areas of focus. The baseline is taken from the current VOC data. |
| Discuss resources that will be needed to complete the pilot implementation plan, including people, time, and projected costs and how the identified resources are effective and beneficial. | – Personnel: Doctors, Nurses, Discharge Coordinators
– Time: 3-6 months for full implementation – Costs: Estimated $50,000 for training, process redesign, and resource allocation |
| Describe training necessary to complete the pilot implementation plan, including the participants and materials required | – Participants: All doctors, nurses, and discharge coordinators.
– – Materials: Training manuals, communication workshops, pain management guidelines. |
| Recommend an actionable strategy, well supported with evidence, to transition any new improvements into daily operational practice | Ensure ongoing monitoring of the process changes and create feedback loops to adjust training as needed. Integrate improvements into hospital policies. |
Conduct an impact assessment of your pilot implementation plan by discussing how the proposed plan may affect the following dimensions and including factors related to the-current state, the transition state, and future state.
| Dimension | Impacts |
| Employees at the organization | Improved communication and workflow will enhance job satisfaction and reduce burnout. Training will empower staff to deliver better care and patient interactions. |
| The community that the organization
serves |
Improved patient satisfaction will result in better health outcomes and potentially reduce the need for readmissions, improving community trust in the hospital. |
| Information management at the organization | Enhanced discharge and patient education protocols will require better data tracking systems to ensure accuracy and follow-up. |
APA Sources:
Ahmadi, A., Bazargan-Hejazi, S., Zadie, Z. H., Euasobhon, P., Ketumarn, P., Karbasfrushan, A., Amini-Saman, J., & Mohammadi, R. (2016). Pain management in trauma: A review study. Journal of Injury and Violence Research, 8(2). https://doi.org/10.5249/jivr.v8i2.707
Jack, B. W., Chetty, V. K., Anthony, D., Greenwald, J. L., Sanchez, G. M., Johnson, A. E., … & Culpepper, L. (2009). A reengineered hospital discharge program to decrease rehospitalization: A randomized trial. Annals of Internal Medicine, 150(3), 178–187. https://doi.org/10.7326/0003-4819-150-3-200902030-00007
Ha, J. F., & Longnecker, N. (2010). Doctor-patient communication: A review. Ochsner journal, 10(1), 38-43. https://www.ochsnerjournal.org/content/10/1/38