Peer Response – Managing Benign Prostatic Hyperplasia (BPH)
Hello,
Thank you for the insightful post on managing benign prostatic hyperplasia (BPH). The comprehensive approach detailed in the post, encompassing diagnostic evaluation, pharmacological management, non-pharmacological interventions, patient education, and follow-up care, provides a well-rounded strategy for managing BPH effectively.
To further enrich the discussion, it is essential to consider the potential benefits of combination therapy in BPH management. Recent studies highlight that combining alpha-blockers like Tamsulosin with 5-alpha-reductase inhibitors, such as Finasteride, can yield superior outcomes in reducing symptoms and slowing disease progression, particularly in patients with larger prostate volumes (American Urological Association, 2021). Notably, this combined therapy is not only highly effective in alleviating symptoms but also reduces the incidence of acute urinary retention and surgical procedures, making it suitable for patients with intermediate to severe BPH.
Moreover, the exploration of emerging minimally invasive surgical options, such as UroLift or Rezūm, offers promising alternatives for patients who may not be appropriate intrants for traditional procedures like transurethral resection of the prostate (TURP), as indicated by Checcucci et al. (2021). These innovative techniques are designed to relieve urinary symptoms with fewer complications and shorter recovery times than more invasive surgeries. In addition, they have the added benefit of preserving sexual function, which is a significant factor in maintaining a patient’s overall quality of life, particularly for individuals concerned about post-surgical impacts.
Finally, while knowledge of BPH is still expanding, studies of genetic and molecular aspects could open up the way to more targeted therapeutic concepts. As such, this changing landscape emphasizes the importance of staying updated with the latest advancements in both medical and surgical interventions, ensuring optimal patient outcomes.
References
American Urological Association. (2021). Benign Prostatic Hyperplasia (BPH) Guideline – American Urological Association. Www.auanet.org. https://www.auanet.org/guidelines-and-quality/guidelines/benign-prostatic-hyperplasia-(bph)-guideline
Checcucci, E., Veccia, A., De Cillis, S., Piramide, F., Volpi, G., Amparore, D., Pecoraro, A., Piana, A., Granato, S., Verri, P., Sica, M., Meziere, J., Carbonaro, B., Piscitello, S., Zamengo, D., Cacciamani, G., Okhunov, Z., Puliatti, S., Taratkin, M., & Marenco, J. (2021). New ultra-minimally invasive surgical treatment for benign prostatic hyperplasia: A systematic review and analysis of comparative outcomes. European Urology Open Science, 33(2), 28–41. https://doi.org/10.1016/j.euros.2021.08.009
ORDER A PLAGIARISM-FREE PAPER HERE
We’ll write everything from scratch
Question 
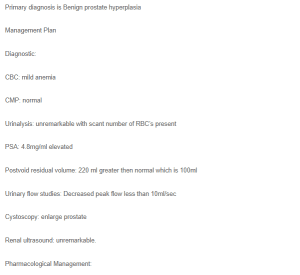
Primary diagnosis is Benign prostate hyperplasia
Management Plan
Managing Benign Prostatic Hyperplasia (BPH)
Diagnostic:
CBC: mild anemia
CMP: normal
Urinalysis: unremarkable with scant number of RBC’s present
PSA: 4.8mg/ml elevated
Postvoid residual volume: 220 ml greater then normal which is 100ml
Urinary flow studies: Decreased peak flow less than 10ml/sec
Cystoscopy: enlarge prostate
Renal ultrasound: unremarkable.
Pharmacological Management:
Medications:
Tamsulosin 0.8mg 1 tab PO daily Dispense: 30 Refill:1 (PDR, 2024).
Consults/Referrals: Urology consultation for possible surgical intervention.
Non-Pharmacological treatment:
Non-pharmacological treatments for benign prostatic hyperplasia (BPH) include lifestyle and behavioral strategies to manage symptoms effectively. Pelvic floor exercises (Kegels) can strengthen bladder-supporting muscles, while dietary adjustments like reducing caffeine and alcohol intake can alleviate urinary issues (Ng et al., 2024). Managing fluid intake by avoiding large amounts before bedtime and staying hydrated to prevent constipation can also help. Regular exercise to maintain a healthy weight, bladder training to extend the time between bathroom visits, and scheduled voiding can further improve symptoms and complement medical treatments.
Client Education:
Patients should be informed about lifestyle changes that can help manage and potentially reduce the need for future BPH surgery. Education on losing weight and better-controlling diabetes can make a difference. Additionally, reducing caffeine and adjusting when you drink fluids can help with troublesome urinary symptoms.
Preventing constipation can help reduce risk factors and improve urinary symptoms.
Patients with BPH should understand how the condition might progress and be given information on different treatment options. These include watchful waiting, medication, and other types of surgery so they can make an informed choice about their treatment.
Educate the patient on the possibility of surgical management for suitable patients, such as patients with persistent or severe BPH refractory to therapy (Lokeshwar et al., 2019). Inform the patient on the expenses of treatment, such as transurethral resection of the prostate and holmium laser enucleation of the prostate.
Follow up:
Follow up with primary care in two weeks. Advised to make an appointment with urology as soon as possible.
References:
Lokeshwar, S. D., Harper, B. T., Webb, E., Jordan, A., Dykes, T. A., Terris, M. K., & Klaassen, Z. (2019). Epidemiology and treatment modalities for the management of benign prostatic hyperplasia. Translational Andrology and Urology, 8(5), 529-539. https://doi.org/10.21037/tau.2019.10.01
Ng, M., Leslie, S. W., & Baradhi, K. M. (2024). Benign Prostatic Hyperplasia. StatsPearls National Library of Medicine. https://www.ncbi.nlm.nih.gov/books/NBK558920/Links to an external site.