Fundamentals of Nursing Care Plan
| Client Data: | ||||||
| Initials: P.B. | Age: 80 years | Gender: Female | ||||
| Weight: | Height: | Race/Ethnicity: Caucasian | ||||
| Diet: Heart-healthy diet | Religion: Baptist | Language Spoken: English | ||||
| Allergies:
Latex Aspirin Sulfadiazine Adhesive bandage |
Marital Status: Married | Code Status: Full code | ||||
| Past Surgeries: N/A | Consults:
|
Social Habits:
Occasional alcohol intake (once or twice per week) Non-smoker |
||||
| Vital Signs: | ||||||
| B/P: | P: | R: | T: | SAO2 sat:
|
||
| 153/74 | 67 | 18 | 97.4 | 99% | ||
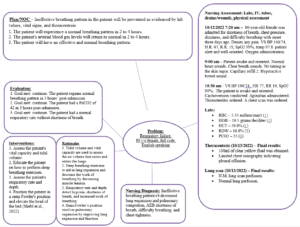
Present History: Admitting Medical Diagnosis:
- Why the client is in the hospital:
Respiratory failure
Admitting Diagnosis Information:
The patient presents with dizziness, difficulty breathing, shortness of breath, and chest tightness.
Definition/Etiology/Pathophysiology:
Respiratory failure occurs when the respiratory system cannot efficiently eliminate carbon dioxide or conduct oxygenation. Respiratory failure is hypercapnic (type Ⅱ) or hypoxemic (type Ⅰ) respiratory failure. Respiratory failure is further described as chronic or acute, depending on the symptoms duration.
Etiology of hypercapnic respiratory failure includes drug overdose, asthma, pulmonary edema, tetanus, cervical cordotomy, poliomyelitis, a chronic obstructive pulmonary disorder, polyneuropathy, porphyria, obesity hypoventilation, acute respiratory distress syndrome, primary muscle disorders, poisonings, myxedema, myasthenia gravis, and primary alveolar hypoventilation. Pneumothorax, bronchiectasis, a chronic obstructive pulmonary disorder, kyphoscoliosis, pneumoconiosis, pneumonia, asthma, pulmonary fibrosis, fat embolism syndrome, obesity, cyanotic congenital heart disease, pulmonary edema, and granulomatous lung disease cause hypoxemic respiratory failure.
Respiratory failure occurs through an abnormality in the central nervous system, alveoli, airways, chest wall, peripheral nervous system, and respiratory muscles. Respiratory failure occurs when there is a malfunction in transporting oxygen to tissues, removing carbon dioxide from the alveoli from blood, and transporting oxygen across the alveoli.
Clinical Manifestations/Signs and Symptoms:
The clinical manifestations of respiratory failure depend on the type of respiratory failure and the underlying disease. Patients diagnosed with respiratory distress present with dyspnea, cyanosis, hypoxemia, tachycardia, hypercapnia, pulmonary hypertension, tachypnea, and neurological manifestations such as anxiety, seizures, and restlessness. Patients with hypercapnic respiratory failure have a PaCO2 of more than 50 mmHg, while those with hypoxemic respiratory failure present with a normal PaCO2 and a PaO2 of less than 60 mmHg. Respiratory failure presents with acute respiratory distress syndrome with sepsis, lung compliance of 40 mL/cm water, pulmonary capillary wedge pressure less than 18 mmHg, and three or 4-quadrant alveolar flooding. Acute respiratory failure presents with several complications. Gastrointestinal complications include gastric distention, diarrhea, bleeding, and pneumoperitoneum, while nutritional complications include malnutrition. Lastly, cardiovascular complications of acute respiratory failure include endocarditis and myocardial infarction. P.B. presents with dizziness, difficulty breathing, shortness of breath, and chest tightness, which are symptoms experienced in respiratory distress.
Medical Management:
Management of hypoxemia focuses on correcting hypoxemia, mechanical ventilation, and patient monitoring. Mechanical ventilation is done to decrease PaCO2 and increase PaO2. Medical management done for P.B. focuses on treating and managing the underlying disease, atrial fibrillation. Amiodarone, atorvastatin, and apixaban are prescribed to control atrial fibrillation. P.B. is administered in the ICU, where oxygen is administered.
Past History/Secondary Diagnosis:
Atrial fibrillation
Definition/Etiology/Pathophysiology:
Atrial fibrillation is an arrhythmia with a rapid and irregular heart rate. Atrial fibrillation commonly leads to the formation of clots in the heart, increasing a patient’s risk of heart failure and stroke. Atrial fibrillation is caused by inflammation such as pericarditis, substance abuse, advancing age, hemodynamic stress such as left ventricular dysfunction, endocrine disorders such as hyperthyroidism, genetics, neurologic disorders such as stroke, atrial ischemia and non-cardiovascular, respiratory causes such as pneumonia. The risk of Atrial fibrillation is higher in individuals above 60 years.
Atrial fibrillation occurs through contractile, electrical, and structural remodeling. The signals in the heart’s upper chambers are uncontrolled, causing the chambers to quiver. Signals transmitted through the ventricles bombard the arterioventricular node, causing irregular and fast heart rhythms (Nesheiwat et al., 2022).
Clinical Manifestations/Signs and Symptoms:
Patients diagnosed with atrial fibrillation usually present with weakness, fatigue, palpitations, lightheadedness, decreased tolerance to physical activity, shortness of breath, and chest pain. P.B. experiences shortness of breath and chest tightness, which are seen in atrial fibrillation. P.B. has respiratory failure, which occurs due to atrial fibrillation (Nesheiwat et al., 2022).
Medical Management
Management of atrial fibrillation focuses on anticoagulation and heart rate control (Nesheiwat et al., 2022). In addition, the treatment plan selection depends on the presenting symptoms and severity. Atrial fibrillation in P.B. is managed using apixaban, atorvastatin, and amiodarone.
List of Medications
| Medication Name/
Frequency |
Indications | Actions | Contraindications | Side Effects | Nursing Implication |
| Apixaban (brand name- Eliquis) 5mg P.O. B.D.
|
§ Prevention of systemic embolism and stroke in non-valvular atrial fibrillation.
§ Treatment of pulmonary embolism. § Prevention of pulmonary embolism after knee or hip replacement surgery. § Treatment of deep venous thrombosis. § Prophylaxis of deep venous thrombosis after knee or hip replacement surgery. § Decreases the reoccurrence of pulmonary embolism and deep venous thrombosis (Agrawal et al., 2022).
|
§ Inhibits factor Xa, leading to blockage of the propagation phase in the coagulation cascade.
§ Inhibits thrombokinase activity and clot-bound and free factor Xa, leading to indirect inhibition of platelet aggregation caused by thrombin (Agrawal et al., 2022).
Therapeutic effects: § Prophylaxis and treatment of thromboembolic events. |
§ Hypersensitivity
§ Active bleeding § Patients with mitral stenosis, mechanical and prosthetic heart valves. § Forty-eight hours before invasive procedures or elective surgery with a moderate or high risk of bleeding § Twenty-four hours before invasive procedures or elective surgery, with a low risk of bleeding (Agrawal et al., 2022)
|
§ Hypersensitivity reaction (allergic edema, rashes)
§ Bleeding § Epistaxis § Rectal hemorrhage § Gingival hemorrhage § Postoperative hemorrhage § Nausea § Hematuria § Bruising § Hemoptysis § Increased levels of gamma-glutamyltransferase, aspartate aminotransferase, and serum transaminases (Agrawal et al., 2022).
|
Assessment:
§ Administer oral-activated charcoal in case of an apixaban overdose. § Monitor the patient for pulmonary embolism and deep venous thrombosis during therapy with apixaban.
Implementation: § Discontinue apixaban 48 hours before invasive procedures or elective surgery with a moderate or high risk of bleeding. § Discontinue apixaban 24 hours before invasive procedures or elective surgery with a low risk of bleeding. § Warfarin should be replaced by apixaban when INR is less than 2. § Discontinue apixaban before initiating therapy with another anticoagulant, such as warfarin (Agrawal et al., 2022).
Patient/Family Teaching: § Advise patient to take apixaban as directed, even if feeling well. § Advise the patient to take a missed dose as soon as possible on the same day. § Educate the patient on signs of bleeding and other side effects. § Advise the patient to take a missed dose as soon as possible on the same day. § Advise the patient to resume taking medication twice daily after a missed dose. § Advise the patient against doubling the dose when there is a missed dose. § If the patient cannot swallow, advise the patient to crush the tablet and suspend it in water (Agrawal et al., 2022). § Advise the patient to take the medication with or without food. § Advise patients to disclose their medication history if they visit a different healthcare provider. § Advise the patient to look for signs of hypersensitivity, such as rashes. § Advise patient against taking over-the-counter medications and herbal medications. |
| Amiodarone 600mg B.D. P.O. for three weeks, followed by 300mg B.D. P.O. for one month, followed by a maintenance dose of 400mg O.D.
|
§ Pulseless ventricular tachycardia/ ventricular fibrillation.
§ Ventricular arrhythmias. § Stable monomorphic ventricular tachycardia. § Polymorphic ventricular tachycardia (Florek & Girzadas, 2022).
|
§ Inhibits adrenergic stimulation, leads to repolarization, prolonged action potential, decreased sinus node function, and atrioventricular conduction (Florek & Girzadas, 2022).
Therapeutic effect: § Management of ventricular arrhythmias.
|
§ Hypersensitivity
§ Cardiogenic shock § Bradycardia with syncope. § Marked sinus bradycardia. Second-degree atrioventricular block (Florek & Girzadas, 2022). § Third-degree atrioventricular block.
|
§ Hypotension
§ Altered memory § Hypothyroidism § Increased levels of aspartate aminotransferase and serum transaminases § Dizziness § Fatigue § Photosensitivity § Headache § Ataxia § Constipation § Sleep disturbances § Congestive heart failure § Hyperthyroidism § Sinoatrial node dysfunction § Bradycardia Hepatitis (Florek & Girzadas, 2022). |
Assessment:
§ Monitor the patient’s heart rate and blood pressure (Florek & Girzadas, 2022).
Patient/Family Teaching: § Advise patient to take amiodarone as directed, even if feeling well.
|
| Atorvastatin 2mg P.O. O.D. nocte | § Prophylaxis or decreased risk of stroke and myocardial infarction.
§ Management of hypercholesterolemia, dyslipidemia, and hypertriglyceridemia (McIver & Siddique, 2022). |
§ Inhibits HMG-CoA reductase, decreasing cholesterol synthesis (McIver & Siddique, 2022).
Therapeutic effect: § Prophylaxis of stroke.
|
§ Hypersensitivity
§ Pregnancy § Lactation § Liver disease § Unexplained elevated transaminase (McIver & Siddique, 2022).
|
§ Diarrhea
§ Arthralgia § Nasopharyngitis § Urinary tract infection § Insomnia § Myalgia § Dyspepsia (McIver & Siddique, 2022). |
Assessment:
§ Monitor the patient’s weight and BMI. § Monitor the patient’s liver function. § Monitor the patient’s serum lipid levels and HbA1c.
Patient/Family Teaching: § Advise the patient to take atorvastatin as directed, even if feeling well. § Advise the patient on dietary modifications and lifestyle modifications to control hypercholeste § Advise the patient to take atorvastatin at night before bedtime (McIver & Siddique, 2022). |
Labs and Diagnostic Tests:
| Labs And Diagnostic Test/Labs | Purpose/ Indications | Normal Values | Client Result | Interpretation of Abnormal Results |
| RBC
|
– To determine blood-related conditions. | 3.8 to 5.2 million/mm3 | 3.35 million/mm3 | Decreased levels may indicate:
– Internal bleeding. – Vitamin B6 deficiency – Vitamin B12 deficiency – Folate deficiency |
| HGB | – To determine blood-related conditions. | 11.6 to 15 grams/decilitre | 10.5 grams/decilitre | Decreased levels may indicate:
– Internal bleeding. – Vitamin B6 deficiency – Vitamin B12 deficiency – Folate deficiency |
| RDW
|
– To detect blood-related conditions and anemia.
|
12 to 15% | 16.8% | Increased levels may indicate:
– Anemia – Internal bleeding |
Nursing Diagnosis Two
Hypertension
Nursing Interventions
Monitor blood pressure and response to medications.
Relacation techniques.
Dietary adjustments, including cholesterol restrictions.
Nursing Rationales
Monitor blood pressure and response to medications to adjust drug dosage.
Relaxation techniques to decrease stress, encourage calmness, and lower blood pressure.
Dietary adjustments, including cholesterol restrictions, to decrease myocardial workload (Iqbal & Jamal, 2022).
Nursing Diagnosis Three
Acute bronchitis
Nursing Interventions
Assess the airway for obstructions.
Chest auscultation.
Position the patient’s bed at 30 degrees.
Nursing Rationales
Assess the airway for obstructions to ensure an efficient gas exchange process.
Conduct chest auscultation to rule out airway obstruction.
Position the bed at 30 degrees to elevate the patient’s breathing pattern and allow normal lung expansion (Singh et al., 2022).
References
Agrawal, A., Kerndt, C. C., & Manna, B. (2022). Apixaban. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK507910/.
Florek, J. B., & Girzadas, D. (2022). Amiodarone. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK482154/.
Iqbal, A. M., & Jamal, S. F. (2022). Essential Hypertension. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK539859/.
McIver, L. A., & Siddique, M. S. (2022). Atorvastatin. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK430779/.
Nesheiwat, Z., Goyal, A., & Jagtap, M. (2022). Atrial Fibrillation. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK526072/.
Shebl, E., Mirabile, V. S., Sankari, A., et al. (2022). Respiratory Failure. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK526127/.
Singh, A., Avula, A., & Zahn, E. (2022). Acute Bronchitis. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK448067/.
ORDER A PLAGIARISM-FREE PAPER HERE
We’ll write everything from scratch
Question 
Fundamentals of Nursing Care Plan
Present History: Admitting Medical Diagnosis:
Why the client is in the hospital:
Medical diagnosis (does not include signs and symptoms)
Admitting Diagnosis Information:
This paragraph should describe the signs and symptoms that caused the patient to visit the hospital. It should not be what the doctor writes word for word. Paraphrase into your words. You may quote the patient.
Definition/Etiology/Pathophysiology:
This paragraph is to define and explain the admitting diagnosis/disease.
This paragraph should describe the etiology. The etiology is what causes the disease.
This paragraph should explain the pathophysiology of the patient’s disease. Pathophysiology describes what the disease does to the body.
Clinical Manifestations/Signs and Symptoms:
This/these paragraphs should explain what the textbook manifestations are and whether the signs and symptoms of the patient are similar or different.
Medical Management:
This/these paragraphs should explain the textbook medical management for the admitting diagnosis of disease. What medical management is currently being done for the patient?
Past History/Secondary Diagnosis:
Name an additional diagnosis that the patient has.
Definition/Etiology/Pathophysiology:
Complete definition/etiology and pathophysiology for the secondary diagnosis as above.
Clinical Manifestations/Signs and Symptoms:
Complete clinical manifestations and signs and symptoms for secondary diagnosis as above.
Medical Management
Complete the medical management of the secondary diagnosis as completed above.
