Differential Diagnoses in a Case of Hypothyroidism
Peer Response
Hello,
Thank you for sharing the detailed and well-researched post. The analysis of Mrs. T. Smith’s symptoms and the proposed differential diagnoses, including hyperparathyroidism, adrenal insufficiency, and chronic renal failure, provides a comprehensive approach to her clinical presentation.
Expanding on the potential diagnoses, it is crucial to consider the interrelationship between hypothyroidism and other endocrine disorders. For instance, hypothyroidism can sometimes coexist with adrenal insufficiency, a condition known as Schmidt’s syndrome, which may complicate the clinical picture and necessitate concurrent management, as indicated by Huecker and Dominique (2023). Furthermore, while chronic kidney disease (CKD) is a pertinent differential, it is essential to recognize that hypothyroidism can contribute to CKD progression by reducing renal perfusion, highlighting the importance of early thyroid function assessment in patients with suspected renal impairment.
Additionally, considering the patient’s sedentary lifestyle and its impact on her metabolic health may also be valuable. Sedentary behavior is a significant risk factor for both hypothyroidism and cardiovascular disease, which may further exacerbate her symptoms of fatigue, weight gain, and overall lethargy (Zúñiga et al., 2024). Encouraging the patient to adopt more active lifestyle habits, such as increasing physical activity beyond walking the dog, could significantly improve her symptoms and overall quality of life.
In conclusion, while the differential diagnoses discussed are highly relevant, integrating the broader endocrine and metabolic implications of hypothyroidism could offer a more holistic approach to Mrs. T. Smith’s case management. This perspective also informs more targeted diagnostic testing and intervention strategies, ultimately leading to a more effective and personalized treatment plan.
References
Huecker, M. R., & Dominique, E. (2023). Adrenal insufficiency. PubMed; StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK441832/
Zúñiga, D., Balasubramanian, S., Mehmood, K. T., Shahad Al-Baldawi, & Gabriel Zúñiga Salazar. (2024). Hypothyroidism and cardiovascular disease: A review. Cureus, 23(46). https://doi.org/10.7759/cureus.52512
ORDER A PLAGIARISM-FREE PAPER HERE
We’ll write everything from scratch
Question 
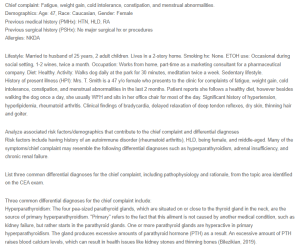
Chief complaint: Fatigue, weight gain, cold intolerance, constipation, and menstrual abnormalities.
Demographics: Age: 47, Race: Caucasian, Gender: Female
Previous medical history (PMHx): HTN, HLD, RA
Previous surgical history (PSHx): No major surgical hx or procedures
Allergies: NKDA
Differential Diagnoses in a Case of Hypothyroidism
Lifestyle: Married to husband of 25 years, 2 adult children. Lives in a 2-story home. Smoking hx: None. ETOH use: Occasional during social setting, 1-2 wines, twice a month. Occupation: Works from home, part-time as a marketing consultant for a pharmaceutical company. Diet: Healthy. Activity: Walks dog daily at the park for 30 minutes, meditation twice a week. Sedentary lifestyle.
History of present illness (HPI): Mrs. T. Smith is a 47 y/o female who presents to the clinic for complaints of fatigue, weight gain, cold intolerance, constipation, and menstrual abnormalities in the last 2 months. Patient reports she follows a healthy diet, however besides walking the dog once a day, she usually WFH and sits in her office chair for most of the day. Significant history of hypertension, hyperlipidemia, rheumatoid arthritis. Clinical findings of bradycardia, delayed relaxation of deep tendon reflexes, dry skin, thinning hair and goiter.
Analyze associated risk factors/demographics that contribute to the chief complaint and differential diagnoses
Risk factors include having history of an autoimmune disorder (rheumatoid arthritis), HLD, being female, and middle-aged. Many of the symptoms/chief complaint may resemble the following differential diagnoses such as hyperparathyroidism, adrenal insufficiency, and chronic renal failure.
List three common differential diagnoses for the chief complaint, including pathophysiology and rationale, from the topic area identified on the CEA exam.
Three common differential diagnoses for the chief complaint include:
Hyperparathyroidism: The four pea-sized parathyroid glands, which are situated on or close to the thyroid gland in the neck, are the source of primary hyperparathyroidism. “Primary” refers to the fact that this ailment is not caused by another medical condition, such as kidney failure, but rather starts in the parathyroid glands. One or more parathyroid glands are hyperactive in primary hyperparathyroidism. The gland produces excessive amounts of parathyroid hormone (PTH) as a result. An excessive amount of PTH raises blood calcium levels, which can result in health issues like kidney stones and thinning bones (Bilezikian, 2019).
Adrenal insufficiency: The lack of the hormones produced by the adrenal glands, which are essential for the body to function, is known as adrenal insufficiency. Adrenal insufficiency can manifest in a variety of ways, from nonspecific, mild symptoms to potentially fatal shock. Androgens, mineralocorticoids, and glucocorticoids are all produced in the cortex. Glucocorticoid and mineralocorticoid deficiencies are mostly caused by destruction or malfunction of the adrenal cortex. Other names for primary adrenal insufficiency include Addison disease and autoimmune adrenalitis (Huecker & Dominique, 2023).
Chronic renal failure: Normally, the kidney is involved in the metabolism, breakdown, and excretion of various thyroid hormones. Thus, it is not unexpected that abnormal thyroid physiology results from kidney dysfunction. Changes in hormone production, distribution, and excretion may be implicated, as may all levels of the hypothalamic-pituitary-thyroid axis (Palmer, 2023). Thyroid function test abnormalities are therefore common in patients with chronic kidney disease (CKD). However, a cautious interpretation of these tests is necessary due to the overlap in symptomatology between hypothyroidism and the uremic syndrome.
Discuss how the three differential diagnoses differ from each other in occurrence, pathophysiology, and presentation. Your discussion should compare and contrast these diagnoses rather than listing them.
The three differential diagnoses differ in pathophysiology and presentation. For hyperparathyroidism, have symptoms such as muscle weakness, fatigue, depression, aches and pains in bones and joints, loss of appetite, nausea, vomiting, constipation, confusion, increased thirst and urination which can be similar to hypothyroidism. However, in hyperparathyroidism this causes high calcium levels in the blood.
In adrenal insufficiency, symptoms may include weakness, fatigue, dizziness, dark skin (Addison’s disease only), bluish-black color around the nipples, mouth, rectum, scrotum, or vagina (Addison’s disease only), weight loss, fluid loss (dehydration), lack of appetite, muscle aches, upset stomach (nausea), vomiting, diarrhea, low blood pressure, low sugar levels, in women, irregular or no menstrual periods. Similar to hypothyroidism, however in adrenal insufficiency the adrenal glands do not produce enough hormones, cortisol and aldosterone.
Individuals with chronic renal failure have symptoms of nausea, vomiting, loss of appetite, fatigue and weakness, sleep disturbance, oliguria, decreased mental sharpness, muscle twitches and cramps, swelling of feet and ankles. In contrast, renal failure result from disease processes in any of the three categories: prerenal (decreased renal perfusion pressure), intrinsic renal (pathology of the vessels, glomeruli, or tubules-interstitium), or postrenal (obstructive) and a state of progressive loss of kidney function (Vaidya & Aeddula, 2021).
Describe relevant testing required to diagnose/evaluate the severity of the three differential diagnoses.
Diagnostic tests to evaluate hyperparathyroidism include routine blood tests measuring the parathyroid hormone (PTH), calcium, 24-hour urine tests, bone density test, x-ray, ultrasound, and CT. For adrenal insufficiency, typically tests include blood and urine tests, checking for levels of the adrenal hormones and ACTH, and imaging tests such as x-ray, ultrasound, and MRI. Lastly, for CKD tests include blood and urine tests, like the GFR and albumin.
Present applicable national guidelines related to diagnosis and diagnostic testing for the differential diagnoses.
According to the U.S. Preventive Services Task Force, there is not enough data to evaluate the advantages and disadvantages of screening for thyroid dysfunction in individuals who are asymptomatic and not pregnant. In patients with Down syndrome, Turner syndrome, subtotal thyroidectomy, type 1 diabetes, autoimmune adrenal insufficiency (Addison disease), radioiodine treatment, radiation therapy of the neck, and use of medications such as amiodarone, lithium, interferons, and rifampin, consider targeted screening at the time of initial diagnosis or medication initiation. Tyrosine kinase inhibitors, phenobarbital, interleukin-2, and immunological checkpoint inhibitors are among the other drugs that could cause screening (Wilson et al., 2021).
A hypothyroidism diagnosis is made on the basis of decreased FT4 blood levels and high thyrotropin, or TSH, in cases of primary causes (thyroid source); in cases of secondary (pituitary source) or tertiary (hypothalamic source) causes, TSH levels can range from normal to low.
References
Bilezikian, J. (2019). Primary Hyperparathyroidism | NIDDK. National Institute of Diabetes and Digestive and Kidney Diseases. https://www.niddk.nih.gov/health-information/endocrine-diseases/primary-hyperparathyroidism
Huecker, M. R., & Dominique, E. (2023). Adrenal Insufficiency. PubMed; StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK441832/
Palmer, B. (2023). Thyroid function in chronic kidney disease. UpToDate. https://www.uptodate.com/contents/thyroid-function-in-chronic-kidney-disease
Vaidya, S. R., & Aeddula, N. R. (2021). Chronic Renal Failure. Nih.gov; StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK535404/#:~:text=Introduction-
Wilson, S. A., Stem, L. A., & Bruehlman, R. D. (2021). Hypothyroidism: Diagnosis and Treatment. American Family Physician, 103(10), 605–613. https://www.aafp.org/pubs/afp/issues/2021/0515/p605.html