Private Problem – Eating Disorder
Section 1: Eating Disorder as a Systemic Issue
Prevalence
Systemic problems are those that occur as a result of the issues endemic in the overall system as opposed to certain individual and isolated factors. According to the National Association of Anorexia Nervosa (2021), about 9 percent of the world’s population is affected by eating disorders. In the US, at least 9 percent of the population, which equates to 28.8 million Americans, are likely to suffer from an eating disorder. Additionally, research shows that African Americans have a lower probability of being diagnosed with anorexia in comparison to white people, even though African American teenagers are said to have a more than 50 percent likelihood of exhibiting eating disorders like purging and binge-eating when compared to white teenagers (ANADA, 2021; Goeree, Ham & Iorio, 2012). Furthermore, Hispanics and Asian Americans are also said to have a higher probability of eating disorders in comparison with non-Hispanic or non-Asian populations. In fact, Uri et al. (2021) claim that Asian Americans who are in college tend to report more elevated degrees of body dissatisfaction as well as negative attitudes regarding obesity compared to non-Asian peers. Eating disorders are also more common among the LGBTQ community as well as persons with disabilities. More recently, it has also been shown that at least 91 percent of adolescent and teenage girls have a great desire to control their weight, and this can be done through crash dieting, self-induced vomiting, or the use of laxatives or diet pills (Ward et al., 2019).
Generally, women, particularly adolescents and younger women, tend to have major issues with eating disorders. The standards of beauty that have been set in the current society, placing emphasis on thinness, have caused many women to go to great lengths in order to remain attractive or beautiful based on societal standards. The graphs below illustrate the depth of this issue.
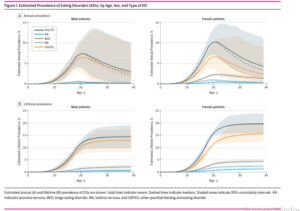
(Ward et al., 2019).
In these graphs, it can be noted that more females, across varying ages, have a higher probability of being diagnosed with eating disorders of all kinds compared to their male counterparts. This is a fact that is backed by the National Institute of Mental Health, as shown in the figure below.
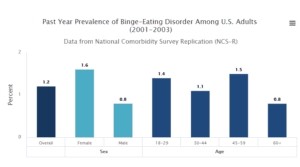
(NIMH, 2021).
American Attitudes Instigating the Problem
The figure above shows that eating disorders are twice as likely to take place among females as among males. There has been a notable increase in eating disorders over the years, and Galmiche (2019) notes a 7.8 percent increase between 2000 and 2018. With a trend of holding women to a higher standard of beauty compared to men, it is not surprising to see an increase in the rate of eating disorders in the country. The issue of obesity is common in the US. Consequently, the issue of body weight or fat-shaming has also increased. Most individuals who get bullied for their weight tend to develop eating disorders. The cultural idealization of thinness and body perfection has caused even children to start being aware of their shapes or bodies at an early age (Muhlheim, 2021). With such negative body images, individuals become dissatisfied with their bodies, causing them to develop problems like low self-esteem, anxiety, and depression. Weight discrimination and bias, particularly when internalized by the individual, could cause eating disorders and could also increase obesity and metabolic syndrome (Vogel, 2019). Issues of fat-phobia and fat-shaming are on the rise. As a cultural and societal phenomenon, particularly in Western nations, fatphobia is viewed as a form of oppression against individuals who are obese or overweight. There are various studies that show that discrimination against individuals who are considered obese or fat has risen since appearance or body discrimination is even observed in healthcare and workplace settings, among others (Monte Nido & Affiliates, 2021). In fact, some scholars claim that discrimination linked to weight is just as prevalent as racial discrimination in the workplace (Monte Nido & Affiliates, 2021). The pervasive belief or negative stereotype that fat people are ugly and lazy has exacerbated issues of obesity as well as eating disorders in the US. Most people rely on the opinions of others regarding their standards of beauty. Social media is a common platform that either enhances or diminishes one’s body satisfaction. For fat people, body shaming on the internet tends to lead them to try and obsessively lose weight through excessive workouts, restriction of calorie intake, and abusing laxatives and diuretics, among others. Once such individuals get positive feedback about weight loss, they are further encouraged to intensify eating disorder behaviors. Anorexia nervosa is considered the most prominent of the eating disorders.
Furthermore, issues like racism, poverty, discrimination, and abuse also tend to trigger eating disorders, as observed in the increase in prevalence among members of minority groups like African Americans, LGBTQ, and Hispanics. These factors cause severe stress, and indulging in eating disorder behaviors could act as a coping mechanism. All these factors reflect that eating disorder is a systemic problem fueled by various environmental and societal factors as opposed to individual factors.
Section 2: Planned Change Model
Engagement Phase
The client, in this case, is assumed to be female, aged 17, and diagnosed with anorexia, an eating disorder. During the engagement phase, the first interaction occurs between the client and the social worker. Skills such as active listening, empathetic responses, eye contact, and empathy are highly recommended as they help build trust and rapport with the client (Department of Social Work, 2017). I will make use of these skills to show the client that I understand and that I am willing to help her through this problem without any form of judgment.
Assessment Phase
This phase entails gathering, analysis, and synthesis of the information to offer a concise picture of the client as well as their strengths and needs. This phase is considered to be the foundation for the subsequent phases (Department of Social Work, 2017). During this phase, I will purpose to identify the concern, in this case, the problem of eating disorder, which has had a negative impact on the client and has prevented her from leading a quality life. I will also assess the nature of the problem and gather the resources and strengths of the client, constantly commending her on these strengths and finding ways to help her exploit the strengths and resources, like a family, that she already has. At the micro-level, I will assess various aspects that could trigger the problem, as stated by the client, including personal attitudes, family, and relations with peers in school. At the mezzo level, I will assess if this is a prominent problem in the client’s group of peers or community and begin thinking of ways of helping them as a whole. At the macro level, I will identify and assess the major triggers for eating disorders rampant in society and begin to think of ways of helping influence policies to deal with the problem.
Planning Phase
This phase involves planning together with the client on the objectives and goals relevant to address the problem (Department of Social Work, 2017). Upon identifying the resources and strengths of the client, it will be important to collaboratively make objectives and goals, and ways of dealing with the problem. I will allow the client to highlight what objectives she would like to achieve to enhance her well-being and independence.
Implementation Phase
During this phase, the social worker, together with the client, execute a plan that is meant to address the areas of concern by actually implementing the stated objectives. Once the objectives have been highlighted, I will collaboratively come up with ways of implementing them and help the client to actually implement those objectives and goals. This might mean offering financial support as she seeks transport services to a psychiatrist.
Evaluation Phase
It is always important to evaluate the client’s progress and make changes to the objectives and goals where necessary in order to attain success. It will be important to have a notebook or journal that helps us track progress, and then together with the client, we will review progress and make changes where necessary.
Termination Phase
Upon realization of the goals, service termination should follow if no additional services are needed. Hopefully, the client will have attained the psychological and emotional capability to deal with whatever would have caused her to have an eating disorder in the first place. Upon the realization of changes in the well-being and progress of the client, termination will occur.
Follow up Phase
In this phase, the social worker needs to reach out to the client and ensure that they are following their goals, making use of their skills, and are improved. By following up with the client, I will be able to assess any additional needs and provide the necessary help where possible. During this phase, I will be able to assess whether the client’s anorexic behavior has lessened or ended, or worsened.
References
ANAD. (2021). Eating Disorder Statistics. https://anad.org/get-informed/about-eating-disorders/eating-disorders-statistics/
Department of Social Work (2017). Introduction to Social Work at Ferris State University. Department of Social Work, Ferris State University
Galmiche, M., Déchelotte, P., Lambert, G., & Tavolacci, M. P. (2019). Prevalence of eating disorders over the 2000–2018 period: a systematic literature review. The American journal of clinical nutrition, 109(5), 1402-1413.
Goeree, M. S., Ham, J. C., & Iorio, D. (2012). Race, social class, and bulimia nervosa. Working Paper, No. 86, University of Zurich, Department of Economics, Zurich.
Monte Nido & Affiliates. (2021). Fat Shaming, Fat Phobia and the Rise in Eating Disorders. https://www.montenido.com/fat-shaming-fat-phobia-rise-eating-disorders/
Muhlheim, L. (2021, January 5). The Connection between Body Image and Eating Disorders. Very Well Mind. https://www.verywellmind.com/body-image-and-eating-disorders-4149424
NIMH. (2021). Eating Disorders. https://www.nimh.nih.gov/health/statistics/eating-disorders
Uri, R. C., Wu, Y., Baker, J. H., & Munn-Chernoff, M. A. (2021). Eating disorder symptoms in Asian American college students. Eating Behaviors, https://doi.org/10.1016/j.eatbeh.2020.101458
Vogel, L. (2019). Fat shaming is making people sicker and heavier. CMAJ, 191(23): E649.
Ward, Z. J., Rodriguez, P., Wright, D. R., Austin, S. B., & Long, M. W. (2019). Estimation of eating disorders prevalence by age and associations with mortality in a simulated nationally representative US cohort. JAMA Network open, 2(10), e1912925-e1912925.
ORDER A PLAGIARISM-FREE PAPER HERE
We’ll write everything from scratch
Question 
Private Problem – Eating Disorder
https://mswcareers.com/generalistinterventionmodel/#:~:text=In%20addition%20to%20offering%20social,intervention%2C%20evaluation%2C%20and%20termination
https://ferrisintroductiontosocialwork.pressbooks.com/chapter/chapter-4-generalist-practice/
The articles at the beginning of Unit 7 illustrate different intervention strategies and theories for social workers. Use those articles, as well as your material from the entire course, to compose your research paper.
Your essay has two sections. Please address each section thoroughly.
Section 1:
Choose a “private problem” that could be indicative of a systemic issue. You are welcome to use the same issue that you discussed in your Unit 5 work.
1) Find a reliable graph or chart that illustrates that this “private problem” could be a systemic issue. In other words, evidence your claim (no Wikipedia, please). Place it in your essay and explain your findings in relation to the issue.
2) Discuss American attitudes, minority treatment, and/or historical events that could contribute to this potential systemic issue.
Section 2:
3) Create a Planned Change Model for that imaginary person with the “private problem”. Remember to address each of the following points of that model (in the readings at the beginning of this unit if you need to refer to them).
* Engagement: Assuming you’ve had no prior knowledge of a person who’s been referred to you with this issue, what would this type of communication look like with a person with this “private problem”?
* Assessment: Examine the private problem through the micro, macro, and mezzo sociological lenses.
* Planning: Once you’ve assessed the situation, how would you go about planning remedies/solutions?
* Implementation: How do you make sure that solutions are implemented? Do you rely on the person who has the “private problem,” or do you do it yourself?
*Evaluation: What controlled environment could you use to evaluate the effectiveness of how well your plans addressed the “private problem”? What does that communication sound like? How do you deal with an issue that was NOT resolved by a potential solution?
* Termination: At what point do you, as a social worker or other professional, decide that your imaginary person’s “private problem” is solved? What are two to three indicators that your imaginary client has felt empowered and learned the skills to achieve social/economic justice?
* Follow-up: How often do you think this should happen? What does this look like?