Suicide Prevention

Int J Environ Res Public Health. 2018 Sep; 15(9): 2028. Published online 2018 September 17. doi: 10.3390/ijerph15092028
World Health Organization. (2019, July 8). Suicide. WHO | World Health Organization. https://www.who.int/health-topics/suicide#tab=tab_1


Int J Environ Res Public Health. 2018 Sep; 15(9): 2028. Published online 2018 September 17. doi: 10.3390/ijerph15092028

National Institute for Mental Health, N. I. M. H. (2015, May 15). NIMH “suicide prevention. National Institute of Mental Health. Retrieved October 25, 2021, from https://www.nimh.nih.gov/health/topics/suicide-prevention.


Self-stigma is a significant mediator in the relationships between experienced stigma and perceived stigma with well-being and recovery variables. Both external and internal influences of stigma work concurrently to affect the recovery and well-being of people with mental illness (Yu, Chio, Mak, Corrigan, & Chan, 2021). Internalized stigma (IS), in addition to the particular mental illness itself, is one of the significant challenges that people with these problems face, and self-esteem, quality of life, hopeful feelings, and stigmatizing experiences, as well as clinical variables, such as depressive symptoms and subjective recovery, are strongly associated with internalized stigma (Del Rosal, González-Sanguino, Bestea, Boyd, & Muñoz, 2021). Other barriers to seeking mental health assistance could be childcare, transportation, or costs.

An example of a religious worldview is Mexican American treatment of mental illness. Although most Latinas/os prefer conventional psychological treatments, such as outpatient and inpatient psychological interventions, they also utilize culturally relevant religious treatments. Examples of these treatments include seeing a priest, using indigenous healers, or seeking faith-based treatment. Levels of stigma toward psychological disorders, however, may be mitigated by the level of education (Hirai, Vernon, Popan, & Clum, 2015). Clergy has historically provided healing; even today, they are an essential resource. Some believe that mental distress can be tinged with spiritual influences and implications (Leavey, Loewenthal, & King, 2016).
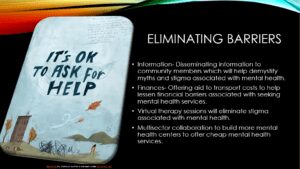
Eliminating barriers, stigma, and shame associated with mental illness is no easy feat. Video portals for therapy sessions have become more available over the past few years. This would eliminate the need for transportation and put less stress on the financial burden and the necessity for childcare. Private practices can help with costs by working with insurance companies to cheapen patient load. Stigmas and shame can be alleviated by informing the public about mental illness. Squashing myths and stereotypes can also help.

Strategies that can be implemented to encourage individuals to reach out for help include ads on websites for easy access to mental health assistance, such as online websites for virtual therapy sessions. Pamphlets can be made in doctor’s or dental offices, schools, and workplaces. Billboards stating things like, “Get help now” or “It’s this easy to get help for mental disorders” may be insightful. Commercials that show real people getting help from doctors and psychologists can also encourage people with psychological illnesses to get help.

Strategies that can be implemented to encourage individuals to reach out for help are to use ads on websites for easy access to mental health assistance, such as online websites for virtual therapy sessions. Pamphlets can be made in doctor’s or dental offices, schools, and workplaces. Billboards stating things like, “Get help now” or “It’s this easy to get help for mental disorders” may be insightful. Commercials that show real people getting help from doctors and psychologists can also encourage people with psychological illnesses to get help. Educational classes or books can also be offered at a low cost.

National Institute for Mental Health, N. I. M. H. (2015, May 15). NIMH “suicide prevention. National Institute of Mental Health. Retrieved October 25, 2021, from https://www.nimh.nih.gov/health/topics/suicide-prevention.
Del Rosal, E., González-Sanguino, C., Bestea, S., Boyd, J., & Muñoz, M. (2021). Correlates and consequences of internalized stigma assessed through the Internalized Stigma of Mental Illness Scale for people living with mental illness: A scoping review and meta-analysis from 2010. Stigma and Health, 6(3), 324–334. https://doi-org.lopes.idm.oclc.org/10.1037/sah0000267.supp
Int J Environ Res Public Health. 2018 Sep; 15(9): 2028. Published online 2018 September 17. doi: 10.3390/ijerph15092028
Hirai, M., Vernon, L. L., Popan, J. R., & Clum, G. A. (2015). Acculturation and enculturation, stigma toward psychological disorders, and treatment preferences in a Mexican American sample: The role of education in reducing stigma. Journal of Latina/o Psychology, 3(2), 88–102. https://doi-org.lopes.idm.oclc.org/10.1037/lat0000035
Leavey, G., Loewenthal, K., & King, M. (2016). Locating the Social Origins of Mental Illness: The Explanatory Models of Mental Illness Among Clergy from Different Ethnic and Faith Backgrounds. Journal of Religion and Health, 55(5), 1607–1622. https://doi-org.lopes.idm.oclc.org/10.1007/s10943-016-0191-1
National Institute for Mental Health, N. I. M. H. (2015, May 15). NIMH “suicide prevention. National Institute of Mental Health. Retrieved October 25, 2021, from https://www.nimh.nih.gov/health/topics/suicide-prevention.
World Health Organization. (2019, July 8). Suicide. WHO | World Health Organization. https://www.who.int/health-topics/suicide#tab=tab_1
Yu, B. C. L., Chio, F. H. N., Mak, W. W. S., Corrigan, P. W., & Chan, K. K. Y. (2021). Internalization process of stigma of people with mental illness across cultures: A meta-analytic structural equation modeling approach. Clinical Psychology Review, 87. https://doi-org.lopes.idm.oclc.org/10.1016/j.cpr.2021.102029
ORDER A PLAGIARISM-FREE PAPER HERE
We’ll write everything from scratch
Question 
This is a Collaborative Learning Community (CLC) assignment using the following scenario:
Suicide Prevention
As a group, you serve as consultants to help create a suicide prevention program for a specific population. For your project, it is assumed you have an unlimited budget and access to any resources you want. A resource list has been provided within the study materials; however, you are not limited to these resources.
Create a PowerPoint presentation and address the following:
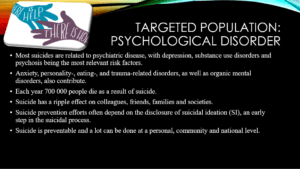
Target Population: Select a target population (e.g., older individuals, individuals with economic problems, veterans, individuals with psychological disorders, LGBTQ, specific ethnic groups, prison populations, medical conditions, substance abuse, or individuals in public safety). Discuss demographics, general risk factors, and warning signs of suicide. Why is this population at greater risk? What are the specific issues or risk factors for this population?
Identification: List ways the program will identify individuals or groups most at risk for suicide (e.g., think beyond self-report surveys and consider including factors such as behavioral cues, psychophysiological measures, and brain scans). How can the identification procedures be implemented in the program to identify more at-risk individuals?
Barriers: What barriers exist for the chosen population? Who might need to seek help? (e.g., stigma, taboos, and shame). What can be done to eliminate these barriers? What role might faith and religion play (e.g., Christian Worldview)?
Strategies: What strategies can be implemented to encourage individuals to reach out for help? What kind of public awareness/education strategies could be helpful?
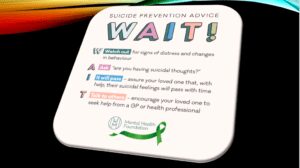
Prevention Plan: What is the plan to help individuals suffering from suicide ideation to prevent suicide? Are there established procedures that are helpful? Are there specific interventions that could be helpful for this population?